As I have already mentioned about the biochemistry of glucose and diabetes briefly on previous post [here] Today I will be sharing a science behind why people having high blood sugar level must go to ophthalmology department for the eye check up or fundoscopic examination ?
Our eye is such a complex organ which helps to visualize the world, colors and even the depth and perception of object. Briefly introducing the anatomy :

Fig: Anatomy of Eye [source]
Cornea: Outermost transparent layer having maximum refractive power. This is the part of eye where maximum laser surgeries are performed. It continues as sclera which is the white part of our eye.
Iris: Coloured part of eye which regulates the amount of light striking the lens via dilating and constricting. (if bright light -> constrict ; dim light -> dilates) Pupil is the dark centered opening in the middle of iris.
Lens: Transparent structure having maximum refractive index which can be replaced if necessary during cataracts or other lens condition. The lens is held by ciliary muscles helping to focus on objects.
Choroid: A layer having numerous blood vessels located between the retina and sclera.
Retina: Nerve layer in back of the eye. It receives light input and converts into electrical signals which is sent through optic nerve to occipital lobe of brain. There are two areas in retina ;
- Macula, which has the most light sensitive cells providing the clarity of vision. Fovea, centered part of macula providing the sharpness of vision
Diabetes has been the major cause for blindness in the people of age 25-65 years in the developed country whereas cataract is still on high grounds in developing country. Diabetic retinopathy (DR) is simply the disease of the retina caused due to high blood sugar level. If one patient had diabetes at age 6 years and other patient had on 12 years, The risk of DR is same for both patients at age 25 as the risk increases only after puberty. Incidence of DR in Female to male ratio is 4:3 and more higher incidence in pregnancy with Diabetes mellitus. DR is prevalent more in poor metabolic control patients. Hypertension, smoking, Dyslipidemia(high lipids in blood) are other major risk factors for DR.
Anti-Diabetic drugs which lowers blood sugar levels; Thiazolidinedione class of drug which includes pioglitazone helps to sensitize insulin are more prone in causing Diabetic retinopathy as conducted using randomized clinical trials.

Fig: Polyol pathway [source]
As sorbitol is produced, it is trapped intracellularly. It has a great osmotic force so tends to drag or absorb more water inwards. Cell swells called as Edema . The enzyme is present in lens which can cause cataract, Schwann cells (Nerve cells) causing Neuropathy, Retinal cells causing Retinopathy. People having increased aldose reductase enzyme due to certain mutations have increased risk to the diseases as mentioned above. Even the accumulation of glycation end products such as sugar + protein and free radical production which causes oxidative damage also increases the risk of DR.
Cellular changes occur where endothelial cells, pericytes(which separates blood vessels and nerve cells also called Blood-brain-barrier)are damaged are compliments are activated. Thickening of the basement membrane occurs. Along with hematological and biochemistry changes, like increased viscosity of blood, platelets adhesiveness (increased ICAM-1), RBC stacking (Rouleaux formation), dyslipidemia, there can be focal ischemia (lack of blood supply), microvascular angiopathy occurs.
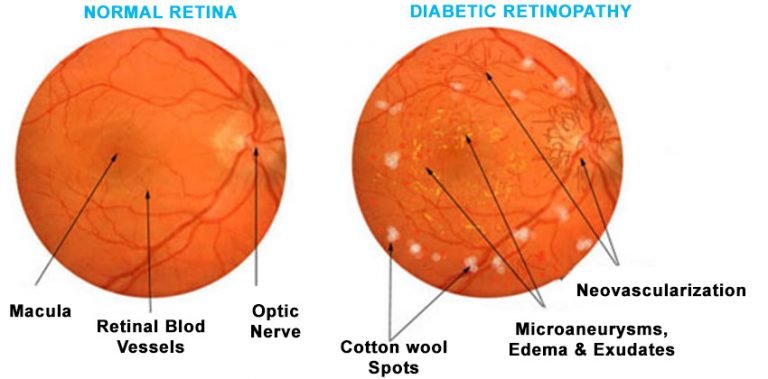
Fig: Normal and Diabetic Retinopathy Fundoscopic image [source]
As vascular auto-regulations are disrupted, there is increased vasoactive substance production which proliferated the capillary cells. Further, it narrows down and Chronic Retinal ischemia occurs. There in increased production of Vascular Endothelial Growth Factor (VEGF) which increases endothelial cell production and increases the vascular permeability. New vessels forms, exudates are formed due to leakage from retinal cells.
He has a blurred, fluctuating vision, floaters or spots in vision , dark or empty vision and last vision loss. Person usually has defect in center part of vision as this does not have significant effects on peripheral part of vision.
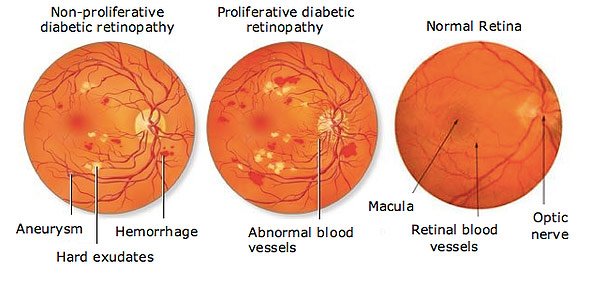
Fig: NPDR and PDR on fundoscopic image [source]
Generally Diabetic retinopathy are classified into two types:
Rather than clinical examination, pathological examinations are more important in classifying DR.
Non-proliferative Diabetic retinopathy (NPDR): This is the early phase of the disease where vessels are weakened and bulges are formed. Some vessels may bleed called as aneurysms. Fluids (proteins) are leaked out and deposited on the layers of retina which can be seen as hard or soft exudates. There is no new vessel formation in this stage. or no angiogenesis is occurring here.
Proliferative Diabetic Retinopathy (PDR) : Damaged blood vessels are closed and new abnormal vessels are growing. This further produce hemorrhage and deposit on the layers of retina. This build up of blood and fluid detach retina causing vision loss (r. Increased fluid causes increased intra-ocular tension resulting in glaucoma.
For controlling of this DR, Asymptomatic cases are usually treated by anti-diabetic drugs and yearly eye examinations are performed whereas, PDR are usually screened for every 2 months. Symptomatic cases are treated with Anti-VEGF medication (bevacizumab, ranibizumab) which is injected into the eye (Vitreous cavity).These stop the proliferation of blood vessels and build up of fluid in the retinal layer. The condition is not curable rather it decreases the occurrence of retinopathy.
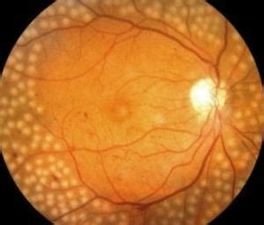
Fig: PRP periphery of retina [source]
Nowdays, Panretinal laser Photocoagulations (PRP) are performed. This procedure photo-coagulates the arising abnormal blood vessels and forms scar. Central part of retina is not performed rather periphery of the retina is usually photocoagulated. Complications like periphery vision is reduced, dark vision or night vision loss is usually complained by the patient.
So this is all for today, hope readers have understood the science behind why ophthalmology check-up or fundoscopic examination is required for diabetic patient.
Reference:
Low vision Aids - Diabetic retinopathy
Mayo clinic - Latest Diagnosis and treatment