WHAT IS HALITOSIS?

When a person has a smelling mouth, regardless of the cause, it is referred to as bad breath.
A more complex term would be Halitosis.
Halitosis is defined as a persistent, unpleasant odour in exhaled breath.
This condition is known to have a large socioeconomic impact as it causes lots of social embarrassment and affect communication.
In itself, it's not a full blown diagnosis, but a pointer to an underlying disease state within and or outside the oral cavity.
A study by P. Eachampati et Al in 2019 shows that 50% to 60% of the world population has experienced this problem. This can eventually lead to loss of self confidence and social stigma.
TYPES
Halitosis is divided into:
- Pseudo Halitosis
- Halitophobia
- Genuine Halitosis
Pseudo-halitosis:
When an obvious breath malodor cannot be perceived but the patient is convinced that he or she suffers from it.
Halitophobia:
This is a term used to describe when a patient still believes that bad breath is present after treatment of genuine halitosis or diagnosis of pseudo-halitosis.
It is a recognized psychiatric condition.
Genuine Halitosis:
This is sub divided into physiologic and pathologic Halitosis.
PHYSIOLOGICAL HALITOSIS
This is halitosis which has no underlying health problems. They are usually transient. Examples include; transient disturbing odor caused by food intake (e.g., garlic, onions, and certain spices), or medications (e.g metronidazole).
The same is true for “morning” bad breath, as habitually experienced on awakening. This malodor is caused by decreased salivary flow and increased putrefaction during the night, and it spontaneously disappears after breakfast or after oral hygiene measures.
PATHOLOGIC HALITOSIS
This is Halitosis as a result of underlying disease state and can be;
- Intraoral: this is when the origin of pathologic halitosis can be found in the oral cavity,
- Extraoral: this can be blood borne and non-blood borne.
Blood borne is the result of bad-smelling metabolites that can be formed or absorbed at any place in the body (e.g., the liver, the gut) and transported by the bloodstream to the lungs.
Non blood borne isn't transported or absorbed by the blood stream.
CAUSES
Causes could be from the mouth (intraoral) or 'others' (extraoral).
Intraoral Causes
These include:
- Tongue coating.
- Poor oral hygiene (accumulation of plaque and calculus).
- Periodontal diseases.
- Dental problems such as tooth decay (caries), food impaction between maligned teeth, accumulation of debris on dentures.
- Dry Mouth (xerostomia).
- Tobacco use
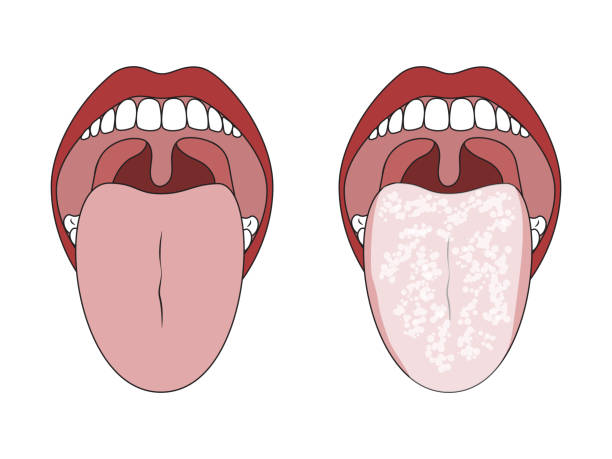
Tongue without a coat vs with whitish coat
Source
 Poor oral hygiene from plaque and calculus accumulation
Poor oral hygiene from plaque and calculus accumulation
Source
The oral bacteria most related to halitosis are gram negative anaerobes such as Actinomyces spp., Bacteroides spp., Eubacterium spp., Fusobacterium spp. These bacteria that are also responsible for periodontitis.
These bacteria release odoriferous substances which give off the odour.
These substances are the volatile sulphur compounds. Others are ammonia and acetaldehyde.
Extraoral Causes
These include:
- Respiratory Infections such as Chronic bronchitis, chronic sinusitis, throat infections, nasal infections and lung diseases.
- Diabetes: Ketone breath is perceived in patients with uncontrolled Diabetes.
- Gastrointestinal disorders such as gastroesophageal reflux disease.
- Kidney Diseases, characterised by give a fishy odor as a result of dimethylamine and trimethylamine.
- Liver diseases, characterised by a sulphur odor.
SYMPTOMS
Complaints of a persistent smelling mouth, which can be confirmed by a third party, which can be verbal or by facial gestures.
DIAGNOSIS
This is done by a dentist.
Diagnosis of Halitosis starts with a detailed history. Patient is advised to avoid taking food substances that predispose to bad breath while coming. Also, confounding doors from perfumes should be avoided.
Medical history of systemic illnesses and ENT (ear, nose and throat) diseases are taken.
The mouth is examined, the tongue for heavy coating, the teeth for accumulation of plaque, calculus and food impaction. Carious teeth are also looked out for.
History of smoking and tobacco use is also gotten.
Examination can be done by the chair side, the different odour from the nasal and oral cavity is checked. This has shortcomings as smell threshold may differ for different people.
A device used in measuring the volatile sulphur compounds, Halimeter is used.
TREATMENT
The choice of treatment will depend on the cause delineated.
- Poor oral hygiene, tongue coating and gingivitis will require scaling and polishing with optimization of oral health practices.
- Periodontal diseases will be treated based on the extent.
- Tobacco cessation
- Management of respiratory Infections and other systemic causes by a Physician.
 What scaling and polishing procedure looks like
What scaling and polishing procedure looks like
Source
Always contact your dentist for the best treatment option.
PREVENTION
It's not enough to know this social killer, how do we stay away from it?
- Good oral hygiene: Brush twice daily, after breakfast and after dinner. Floss twice daily and brush your tongue too.
- Do scaling and polishing once in 6 months. See a dentist.
- Quit smoking.
- Take good care of your denture, do not sleep with it at night.
- Consult with your Dentist and primary healthcare provider.
I hope you learnt something from this piece. Got questions or contributions? Let's interact in the comments.
References:
CML Bollen, T Beikler - International journal of oral science, 2012 - nature.com
https://www.nature.com/articles/ijos201239Hampelska K, Jaworska MM, Babalska ZŁ, Karpiński TM. The Role of Oral Microbiota in Intra-Oral Halitosis. Journal of Clinical Medicine. 2020; 9(8):2484. https://doi.org/10.3390/jcm9082484
(PDF) Prevalence of self-reported halitosis and associated factors among dental patients

